

Introduction: C-reactive protein (CRP), the most commonly used clinical indicator of inflammation, plays an important role in disease diagnosis and efficacy evaluation. Recent studies identified elevated CRP level and CRP kinetics, dynamic change of CRP level throughout treatment, were associated with decreased clinical outcome in some malignancies. Because of increased catabolism and the reduce of hepatic synthesis, albumin is oppositely associated with inflammatory. CRP/ albumin ratio (CAR) is a novel and superior prognostic factor involving inflammatory and nutritional factors in various cancers. However, the prognostic role of CRP, CRP kinetics and CRA in B-cell chronic lymphoproliferative diseases (B-CLPD) were not well characterized yet. Our study focused on the prognostic role of CRP, CRP kinetics and CRA in newly diagnosed B-CLPD.
Methods: In total, 243 newly diagnosed B-CLPD patients from January 2012 to December 2019 at the Shandong provincial hospital in China were analyzed for overall survival (OS) and disease-free survival (DFS), depending on CRP, CRP kinetics and CRA. OS and DFS were determined by Kaplan-Meier curves and log-rank test. Cox proportional analysis was performed to examine the prognostic significance of clinicopathological variables in multivariate analyses.
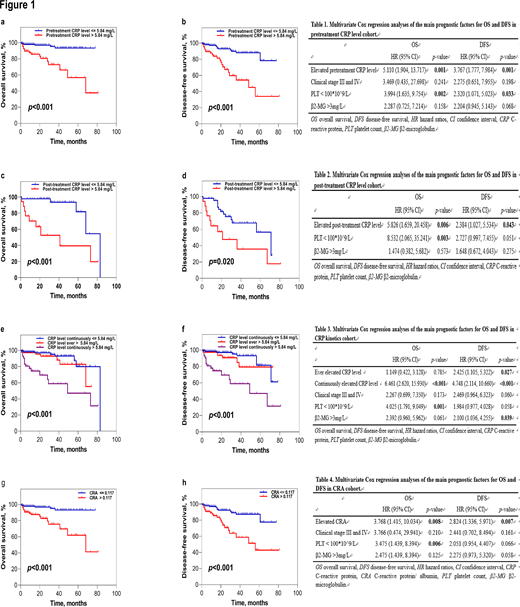
Results: The five-year OS of patients with elevated pretreatment CRP level (94.3% vs. 56.7%, p<0.001) (Figure 1a), elevated post-treatment CRP level (81.7% vs. 39.4%, p<0.001) (Figure 1c), continuously elevated CRP level during the whole treatment process (80.0% vs. 47.1%, p<0.001) (Figure 1e) and elevated pretreatment CRA level (93.1% vs. 61.9%, p<0.001) (Figure 1g) were shorter than normal patients, respectively. Compared to normal patients, the five-year DFS of patients with elevated pretreatment CRP level (88.0% vs. 33.9%, p<0.001) (Figure 1b), elevated post-treatment CRP level (56.4% vs.35.7%, p=0.020) (Figure 1d), ever-elevated CRP level (62.9% vs. 35.3%, p<0.001) (Figure 1f), continuously elevated CRP level during the whole treatment process (80.2% vs. 35.3%, p<0.001) (Figure 1f) and elevated pretreatment CRA level (87.3% vs. 42.8%, p<0.001) (Figure 1h) were shorter, respectively.
Multivariate analyses identified that elevated pretreatment CRP level (HR: 5.110, p=0.001) (Table 1), elevated post-treatment CRP level (HR: 5.826, p=0.006) (Table 2), continuously elevated CRP level (HR: 6.461, p<0.001) (Table 3) and elevated pretreatment CAR (HR: 3.768, p=0.008) (Table 4) had association with worse OS. Likewise, elevated pretreatment CRP level (HR: 3.767, p=0.001) (Table 1), post-treatment CRP level (HR: 2.384, p=0.043) (Table 2), ever-elevated CRP level (HR: 2.425, p=0.027) (Table 3), continuously elevated CRP level (HR: 4.748, p<0.001) (Table 3) and elevated pretreatment CAR level (HR: 2.824, p=0.007) (Table 4) were in independent significance with worse DFS.
Conclusions: We demonstrate that CRP level, CRP kinetics and CAR could be potential prognostic indicators with independent significance in patients with B-CLPD. CRP and CAR make an implementation for prognostic evaluation more easily and effectively in B-CLPD patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal